SVT on ECG: why does it have to be so confusing (for nurses & nursing students)?
The short answer? It doesn’t. Let’s try to break SVT down in as few words as possible:
Understand that SVT is an umbrella term that describes many different rhythms originating above the ventricles.
What is SVT?
Supraventricular tachycardia (SVT) is by definition, any tachycardia (>100 bpm; no, not >150 bpm) originating above (supra) the ventricles (in this case, above the Bundle of His). Because of this, these rhythms have something in common: a narrow QRS complex. We commonly referred to these as narrow complex tachycardias, excluding aberrant conductions. The QRS is narrow because the impulse is being passed down the natural conduction pathway from above (supra) to the ventricles. When an impulse originates from within or at the level of the ventricles the QRS is wide and ugly; partly because the ventricles themselves are thick, and muscle takes longer to conduct relative to the specialized pacemaker cells along the normal conduction tract [this is why premature ventricular contractions (PVCs) are early, wide, and ugly.]
What does it mean?
This is where the water gets a little muddy. Let’s review:
Many sources use the term SVT to describe a regular, narrow complex tachycardia, with a rate >150 bpm, and no discernible P waves
What they fail to mention however, is that in these cases they’re often referring to particular “re-entry” tachycardias (think of a circuit stuck inside a loop that has trouble escaping. These are the classic SVTs that **typically respond to adenosine (in addition to others but let’s keep it simple here).
AV nodal re-entry tachycardias (AVNRT) and Atrio-ventricular re-entry tachycardias (AVRT) are what this describes. See the image below.

Our full definition of SVT would also then include any tachycardias (>100 bpm) originating above the ventricles. These rhythms may be regular and include for example:
Sinus tachycardias
Focal atrial tachycardias
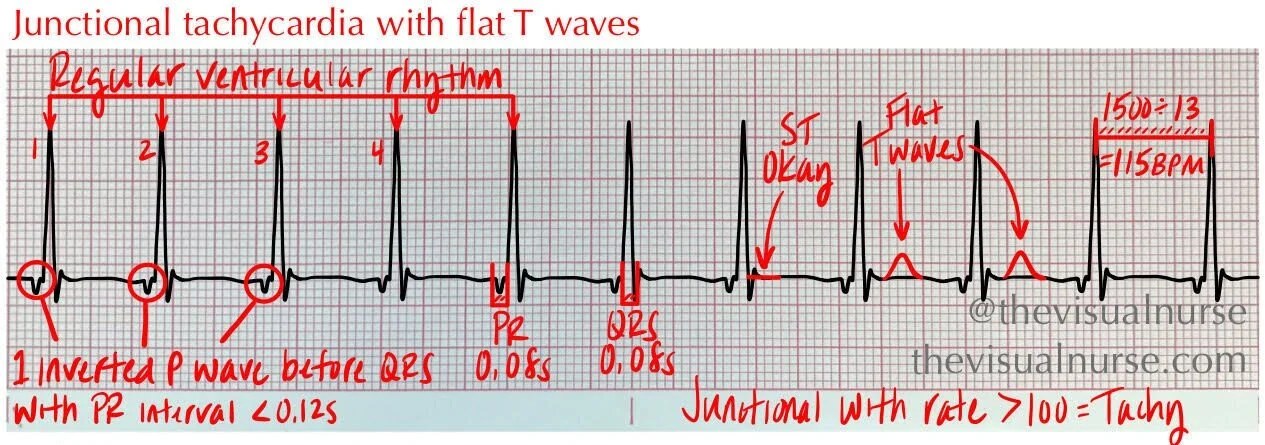
Junctional tachycardias
Atrial flutters >100 bpm with fixed ratio


But they can also be irregular, for example:
Atrial flutters >100 bpm with variable conduction ratio
Rapid (>100 bpm) atrial fibrillation
Multifocal atrial tachycardias


Why should I care?
Q: “Okay, so this is great information and all but what do I do with it?” …
A: Well, in my humble opinion you should receive the term “SVT” with a grain of salt and understand that 99.99999999… percent of the time those who use this nomenclature are referring to a:
Regular
Narrow complex
Tachycardia
With a rate >150 beats per minute and
No discernible P waves (as below).



Just keep in mind that SVT is actually an umbrella term that describes much more than just AVRTs and AVNRTs. Hope this helps!
-Tyler